(Prepared by Dr Gabriel Castro)
61 y/o woman, presented with hyperthyroidism symptoms. TSH: < 0,02 mU/ml (NV
0,43-3,7), T4L: 2,66 ng/dl (NV 0,87-1,5) y T3L: 8,79 pg/ml (NV 2,6-3,7). I 131
uptake at 2 hrs: 13% (NV:2-9%) and at 24 hrs: 54% NV: 7-26%. She underwent a
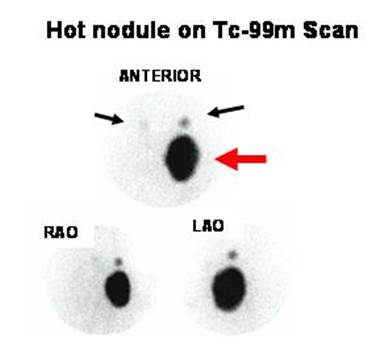
Tc99m pertechnetate Thyroid scan that showed a big round focus of intense Tc99m
uptake that comprised the inferior and mid portion of left thyroid lobe (red arrow). The rest of
thyroid parenchyma is suppressed, save two small additional functioning nodules
or colloid cyst one in the upper right lobe and the other in the left upper lobe (black arrow). Autonomously functioning toxic adenoma
(Plummer's disease) was diagnosed and I 131 treatment was planned.
Thyroid scintigraphy provides
molecular-based information on nodular function, and is able to prove the
presence of autonomously functioning thyroid tissue (hot nodule) (1).
Autonomously functioning toxic adenomas are a common cause of hyperthyroidism.
“Single or multiple doses of radioiodine can successfully treat toxic adenomas
with a low rate of hypothyroidism and considerable nodule-volume reduction” (2).
References:
1 J. Meller, W. Becker. The continuing importance of thyroid scintigraphy in the era of high-resolution ultrasound. Eur J Nucl Med (2002); 29 (Suppl. 2): S425–S438.
2 Erdoğan MF, et al. Effect of radioiodine therapy on thyroid nodule size and function in patients with toxic adenomas. Nucl Med Commun. 2004 Nov; 25(11): 1083-7.
3
Degrossi OJ et al. Diagnóstico del Bocio Nodular, p: 691-176 in: Medicina Nuclear Aplicaciones Clínicas. Eds: I. Carrio -
P. González. Editorial Masson, Barcelona España, 2003.
Home Index Thyroid Scintigraphy Clinical Applications Hot Nodule Menu