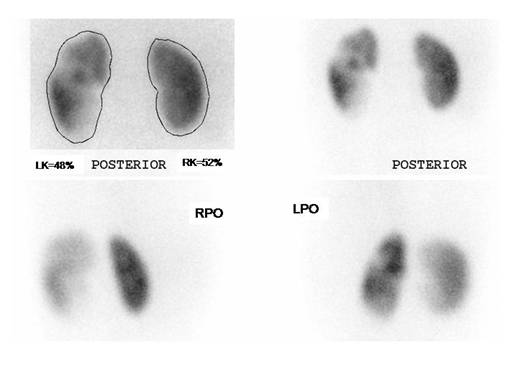
UNILATERAL Acute Pyelonephritis
Child 7 y/o, fever for 4 days. See left kidney enlarged, with multiple focal defects all over the organ. Relative function is normal and so is right kidney.
Renal Scintigraphy is very sensitive to detect acute parenchymal infections, over 90 %. It may be positive with negative ultrasound or urine test and culture. On the other hand a normal scan almost rules out acute infection.
Some authors have proposed the use of MAG-3 renogram to shorten the study and diminish the radiation dose, with similar sensitivity (2,3). However, this needs further evaluation and so far DMSA keeps being the procedure of choice to detect APN and kidney scars at follow up.
Mantadakis et al. proposed that in children with culture-proven UTI, a serum procalcitonin (PCT) value >0.5 ng/mL predicts reasonably well the presence of renal parenchymal involvement, as evidenced by DMSA scintigraphy. PCT may aid in the identification of children with UTI, necessitating more intense evaluation and management (4). It is clear that the standard for acute renal infection is the DMSA scan. However, PCT could be useful to predict scars if the value is high or its course shows increment, at the time of the acute infection episode (5).
Kotoula et al reported that PCT is superior to conventional inflammatory markers for prediction of renal parenchymal inflammation in pediatric first urinary tract infection (6). DMSA scan was used as the confirmatory procedure.
References:
1 Rossleigh MA. Renal infection and vesico-ureteric reflux.Semin Nucl Med. 2007 Jul;37(4):261-8.
2 Sfakianakis GN, Cavagnaro F, Zilleruelo G, Abitbol C, Montane B, Georgiou M,Ezuddin S, Mallin W, Sfakianakis E, Strauss J.Diuretic MAG3 scintigraphy (F0) in acute pyelonephritis: regional parenchymal dysfunction and comparison with DMSA. J Nucl Med. 2000 Dec;41(12):1955-63.
3 Grbac-Ivanković S, Smokvina A, Girotto N, Licul V. Initial presentation of scintigraphic changes during the first episode of acute pyelonephritis in children: simultaneous evaluation with MAG3 and DMSA. Nuklearmedizin. 2007;46(4):129-34.
4 Mantadakis E, Plessa E, Vouloumanou EK, Karageorgopoulos DE, Chatzimichael A, Falagas ME.Serum procalcitonin for prediction of renal parenchymal involvement in children with urinary tract infections: a meta-analysis of prospective clinical studies. J Pediatr. 2009 Dec;155(6):875-881.e1. Epub 2009 Oct 21.
5 Bressan S, Andreola B, Zucchetta P, Montini G, Burei M, Perilongo G, Da Dalt L. Procalcitonin as a predictor of renal scarring in infants and young children. Pediatr Nephrol. 2009 Jun;24(6):1199-204. Epub 2009 Feb 10.
6
Kotoula A, Gardikis S, Tsalkidis A, Mantadakis E, Zissimopoulos A, Deftereos S,
Tripsianis G, Manolas K, Chatzimichael A, Vaos G. Comparative efficacies of
procalcitonin and conventional inflammatory markers for prediction of renal
parenchymal inflammation in pediatric first urinary tract infection.Urology.
2009 Apr;73(4):782-6. Epub 2009 Jan 18.